20 June 2023: Database Analysis
COVID-19 Pandemic and Healthcare Communication: A Patient-Centric Evaluation of Treatment and Diagnostic Procedures in Poland
Zbigniew IzdebskiDOI: 10.12659/MSM.940227
Med Sci Monit 2023; 29:e940227






Abstract
BACKGROUND: The COVID-19 pandemic necessitated swift and often abrupt changes in healthcare practices, significantly influencing treatment and diagnostic procedures. This study aimed to gauge patient perceptions regarding these changes and their overall impact on the treatment and diagnosis process (ITDP).
MATERIAL AND METHODS: In March 2022, we conducted a cross-sectional online survey among 1860 Polish residents (mean age: 48.82±16.57 years), who had accessed medical services within the preceding 24 months. We employed a binary logistic regression model to pinpoint independent factors contributing to a wholly negative perception of the pandemic's influence on the ITDP.
RESULTS: Around 64.3% of respondents perceived the ITDP during the pandemic negatively, with 20.8% reporting mixed impacts. Of 22 factors considered, 16 were significantly associated with ITDP perceptions in univariate analyses, and 8 qualified for the final multivariate model. The most potent predictors of negative ITDP perceptions included impeded communication with medical personnel due to the emphasis on COVID-19 (OR=2.82; 95% CI: 2.04-3.90) and worsening family financial circumstances during the pandemic (OR=2.03; 95% CI: 1.26-3.27). Other significant predictors comprised viewing remote services as a hindrance to medical communication, higher education, and use of self-funded private healthcare.
CONCLUSIONS: Our findings confirm that negative perceptions of the ITDP during the COVID-19 pandemic are associated with the remote delivery of medical services and communication challenges. These insights underscore the need to improve these domains for better healthcare delivery amid ongoing or future health crises.
Keywords: Communication, COVID-19, Diagnostic Services, Health Services Accessibility, Patients, Poland, Humans, Adult, Middle Aged, Aged, Pandemics, COVID-19, Cross-Sectional Studies, Delivery of Health Care, Patient-Centered Care, COVID-19 Testing
Background
The COVID-19 pandemic spread extremely fast and required the implementation of interventions that were often chaotic or temporary and caused drastic changes in the daily lives of individuals and families [1]. The pandemic period made it abundantly clear how important the pillar of population policy is for improving population health and reducing mortality [2,3].
According to official statistics, from March 4, 2020 to July 30, 2022, 6 069 016 people in Poland were infected with the SARS-CoV-2 virus [4]. During the pandemic period, the phenomenon of excess mortality, defined as mortality significantly exceeding the level expected under standard conditions, was recorded in Poland [5]. The scale of the phenomenon was indicated in the latest report on the health situation of the Polish population and was also highlighted by experts participating in a debate on the consequences of the pandemic, which was held at the Supreme Chamber of Control (NIK) in October 2022 [6].
It has been emphasized that most health systems began to implement measures to suppress the spread of the virus after the first phase of “underestimating” the COVID-19 pandemic, initially in a less and then in a more coordinated manner [7]. With regard to Poland, significant factors that hindered the fight against the pandemic were earlier organizational problems and the lack of legislative-regulatory solutions, which were intensified by the lack of the widespread use of system solutions that had gradually been developed in other countries [8]. The fact that the healthcare system in Poland has failed to cope with numerous challenges over many years has impacted its perception by patients. More than half of Polish people declare that they are definitely dissatisfied or rather dissatisfied with how healthcare functions in the country [9]. Poland also has the lowest number of practicing physicians (2.4) and nurses (5.1) per 1000 inhabitants in the European Union [10] and suffers from the misallocation of personnel resources, which is an even greater problem. During the pandemic, staff shortages in healthcare became more pronounced, which was not solved by offering higher salaries.
It is noteworthy that even before the COVID-19 pandemic, in 2018, Poland was ranked 4th from the bottom (ahead of Albania, Romania, and Hungary) in the European Consumer Health Index (EHCI), in which individual countries are compared in terms of securing patient rights, waiting times for treatment, treatment outcomes, the scope and coverage of services, and the prevention and availability of medicines [11]. Importantly, in the first year of the COVID-19 pandemic (2020), there was an unprecedented reduction in the frequency of hospitalizations among Polish citizens, and the year was characterized by a significant deterioration in care for patients with cardiovascular diseases (both inpatient and outpatient) and an adverse impact on the ability to combat chronic infectious diseases (particularly HIV, HCV, and HBV infections), as well as a significant decline in the diagnosis rates of malignant neoplasms [12].
The National Health Program for 2021–2025 emphasized that the COVID-19 epidemic, along with the epidemic of chronic non-communicable diseases and the process of population aging, has caused a negative synergy effect [13]. The long-term consequences of neglect during the pandemic period are often considered as health debt. Health debt is defined as the accumulated impact of changes in health behaviors, including the utilization of healthcare, during the pandemic that have caused long-term negative effects on health and chronic diseases [14]. Serious effects have been seen in the aforementioned area of ongoing diagnosis, but attention has also been drawn to changes in diet and the less frequent adoption of health-promoting behaviors, including preventive screenings [15]. In the long term, both the abandonment of secondary and primary prevention strategies could affect the health of the population. However, this health debt problem has been taken seriously and actions are being taken to reduce it on an ongoing basis.
The Patient Rights Ombudsman’s Report [16] has shown that the exclusion of some general hospitals and their transformation into COVID-19-dedicated hospitals has made it much more difficult for patients using these units to access health services and has heightened their concerns about the continuity of treatment. At the same time, in January-September 2020, the Office of the Patient Rights Ombudsman received 6952 individual written complaints or requests, whereas during the same period in 2019, there were 4809 requests, demonstrating an increase of more than 44%. The reported complaints predominantly concerned the aforementioned restrictions of the availability of healthcare services. Some of the submissions noted patient concerns about due diligence in telemedicine. In addition, the spread of the SARS-CoV-2 virus has affected the use of medical services in Poland. Comparing data from 2018 and July 2020, a CBOS report [17] found that there was a clear increase in the overall number of people who did not receive any treatment and examinations (from 12% to 30%), while there was a definite decrease in mixed-funded medical services both within and outside the general health insurance (from 48% to 28%).
The aforementioned issues and areas of concern undoubtedly influenced patient perceptions of the treatment and diagnostic process during the COVID-19 pandemic, as the quality of services provided at treatment facilities is a fundamental condition for their effectiveness. Patient expectations are clearly and strictly defined and patient evaluation, although subjective, is one of the measurable indicators of the quality of treatment facilities [18]. Patient-oriented communication, which positively influences satisfaction levels [19], as well as adherence to medical recommendations and treatment outcomes [20], also remains an important element in the perception of service quality. The COVID-19 pandemic affected the relationship between healthcare workers and patients due to the potential risk of transmitting the SARS-CoV-2 virus. In particular, using personal protection equipment and maintaining social distancing were recommended to reduce the risk [21]. However, masks and other personal protective equipment made it difficult to maintain eye contact with patients, thus reducing the effectiveness of communication [22]. It also is worth considering that covering the face disrupts nonverbal communication, which accounts for almost 93% of interpersonal communication [23]. In addition, social distancing, which prevented physical proximity and contact through touch, is another potential barrier to nonverbal communication, and in one study, 96.1% of patients reported that the use of social distancing affected their relationships with physicians [24]. A tap on the shoulder, a touch on the hand, or a handshake from medical professionals are all expressions of support and empathy [25], which were made impossible during the pandemic period. In addition, doctors limited the time they spent with patients in order to effectively reduce the transmission of the virus [26]. The aforementioned changes in the way healthcare workers provided services undoubtedly affected the effectiveness of their interactions with patients.
Implemented at the University of Warsaw, a project on the humanization of medicine and communication between healthcare workers and patients has provided a unique source of information on patient perceptions of the treatment and diagnostic process during the COVID-19 pandemic. The original aim of this project was to look at the subjective evaluation of this process from the perspective of the restrictions associated with the pandemic. The compiled research report [27] indicated that the predominant evaluation was exclusively negative. Difficult contact with a doctor was the most frequently cited negative effect. The empirical material collected in March 2022 allowed for a broader analysis of the determinants of patient perception of the treatment and diagnosis process during the pandemic. Focusing on communication barriers that were directly and indirectly related to the imposed restrictions, the personal characteristics of patients and the conditions under which medical services were provided during this period were also included among the determinants.
This paper aims to present an assessment of the impact of the COVID-19 pandemic on the treatment or diagnostic process (ITDP) and identify the main factors affecting ITDP perception.
The following detailed research questions were formulated:
Material and Methods
SAMPLE:
The survey was conducted as part of a project implemented by the University of Warsaw with funding from the Medical Research Agency, entitled “Humanization of the treatment process and clinical communication between patients and medical personnel before and during the COVID-19 pandemic”. The field study was carried out by the Interactive Research Center between March 2 and March 20, 2022. The inclusion criteria were being aged 18 or over and the use of medical services related to treatment or diagnosis within the previous 24 months. The exclusion criteria included working in the health sector, only obtaining services in private medical centers and limiting contact with health services during this period due to vaccinations, medicine prescriptions, or other administrative actions [27].
The sample was nationwide and stratified by gender, age, education level, region, locality size, the format of the medical service (ie, face-to-face contact, remote consultation) and its location (ie, at a hospital, clinic). To improve the representativeness of the results we applied stratified sampling with non-equal sample sizes from each stratum. Samples of 1000 respondents are recommended for social and opinion polls; we have significantly exceeded these guidelines. The objective was to obtain target sample with a specified structure, taking into account the structure of the Polish population.
The records accepted for the final database included 2050 adult respondents, 1860 of whom were able to assess the impact of the COVID-19 pandemic on the treatment and diagnosis process. The analyzed group included 930 men and 930 women. The mean age of the respondents was 48.82 (SD=16.57) years and the proportions of those under 30 and over 65 were 14.0% and 22.1%, respectively. The residents of rural regions accounted for 36.1% of the total, while residents of large cities (ie, cities with over half a million residents) accounted for 13.1%. A total of 1848 people who responded to the question on working status (50.9%) were employed. Education level was re-coded from 12 into 3 categories: below secondary (22.8%), secondary (39.0%), and above secondary education (38.2%). Within the selected sample, 1346 people (72.4%) were currently in a stable relationship, of whom 77.0% were married and 22.7% were in informal relationships (0.3% [5 people] refused to answer). The economic situation of the respondents was described using subjective indicators, current assessments, and changes during the pandemic. The question on change was answered by 1765 respondents, but the economic situation of participants only improved in 87 cases (4.9%) and remained unchanged in 998 (56.6%), while in 680 (38.5%) cases, it worsened and significant deterioration was declared by 7.6% of respondents.
We verified that respondents eliminated from this study because the lack of data on ITDP did not differ from those included in terms of the above basic characteristics.
The thematic scope of the questionnaire, the research procedure, and the mode of obtaining participant consent were all approved by the research ethics committee at the Faculty of Education, University of Warsaw (decision number 2021/8).
RESEARCH TOOLS AND INDICATORS:
The subjective assessment of the impact of the COVID-19 pandemic on ITDP was considered the main dependent variable in this study. The questionnaire included the following question:
In accordance with the aim of the study, the ITDP was analyzed first and foremost within the context of restrictions to HCW-patient communication that were related to the COVID-19 pandemic. Respondents responded to the 7 communication difficulties cited below on a 4-point scale, from
In addition to the above difficulties, other factors that potentially affected the ITDP were divided into 2 groups:
STATISTICAL ANALYSIS:
The percentage distribution of the responses to each question was provided as a sample characteristic. The associations between the categorized variables were tested using the chi-squared test of independence. In a univariate analysis of the relationships between pandemic restrictions and the ITDP, Somers’ d coefficient was used as a measure of effect size, taking the impact of the pandemic as the dependent variable. This is a measure of the relationship between 2 ordinal characteristics obtained from a contingency table. In this study, a positive value meant that the more restrictions, the more often negative and neutral effects of the pandemic were recorded.
As part of the multivariate analysis, a binary logistic regression model was estimated to identify independent factors influencing the exclusively negative assessment of the pandemic’s impact on the treatment and diagnosis process. Factors that were found to be significant in the previous univariate analyses were included in the model and the selection of the final model was based on the Wald test. The results were presented as beta parameters with their SE, odds ratios (ORs), along with 95% confidence intervals (95% CIs), according to the order in which the variables were entered into the model. Once the final model was obtained, it was recalculated using the simple entry method to reduce the number of missing data. SPSS v.27 (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) software was used to analyze the data. All significance levels were set as
Results
RESPONDENT HEALTH AND THE TREATMENT UNDERTAKEN DURING THE COVID-19 PANDEMIC:
The health status of the respondents was described using measures of subjective evaluation and chronic disease status (Table 1). Almost half of the respondents (47.3%) assessed their health as good or very good, but 1 in 5 (21.8%) assessed their health as poor. Long-term health conditions that had been diagnosed by a doctor and lasted at least 6 months were declared by 60.8% of respondents, but 7.8% were unable or unwilling to indicate their chronic disease status.
The remaining information presented in Table 1 relates to treatment received during the 24 months preceding the survey, which included the COVID-19 pandemic period. Most often, patients received medical services at a hospital, outpatient clinic, or specialist’s office. Combining co-occurring responses about inpatient treatment, 677 respondents (36.4%) were patients in an ED or hospital ward for 24-hour care or 1-day clinics. The predominant form of care (54.0%) was a combination of public healthcare (National Health Fund, NFZ) and private care. Public healthcare (NFZ)-only treatment was used by 43.2% of respondents. Private treatment was mostly self-funded, as declared by 77.9% of respondents who received private care. A small percentage of patients (1.7%) had exclusively remote contact with healthcare professionals during the COVID-19 pandemic. Patients were most likely to obtain medical services via face-to-face consultations (58.6%), although the percentage of patients who received both remote and face-to-face consultations was also high (41.4%). Patients also reported which medical services they had used in the past 24 months, with the option to mark multiple answers. Overall, 1 in 10 respondents (10.9%) only marked 1 answer. Patients most often reported receiving medical consultations (89.4%) and preventive or diagnostic services (69.7%). A significant percentage (63.4%) underwent immunizations during the pandemic period but according to the criteria, vaccinations were not their only contact with healthcare services.
The scope of the questionnaire did not make it possible to determine whether the respondents had the SARS-CoV-2 virus at the time of the survey since only some of them had been tested and were sure of their results. However, they were also asked about the place of treatment, which made it possible to identify people who did not have COVID-19 or were asymptomatic (59.5%), those who self-treated at home (27.6%) and those who were under the care of a doctor or in a hospital (12.9%). Within the study sample of patients, 29 cases of hospital treatment related to the SARS-CoV-2 virus were recorded.
DIFFICULTIES IN COMMUNICATION AND RELATIONSHIPS WITH HCWS DURING THE COVID-19 PANDEMIC:
Table 2 shows the patient opinions on difficulties in communication and relationships with HCWs during the COVID-19 pandemic, which were broken down into 7 potentially hindering factors. Chaotic information, the inability of patients to communicate with their relatives, and the increased focus on medical problems associated with COVID-19 were identified as the main hindering factors. In turn, the need to maintain social distancing was identified as a hindering factor relatively less frequently.
ITDP AND SELECTED DETERMINANTS:
In the surveyed group of 1860 patients who were treated during the COVID-19 pandemic, negative opinions prevailed (1196 respondents, 64.3%). Only 41 people (2.2%) rated the impact of the pandemic as only positive, while 388 (20.9%) noticed positive and negative effects. Additionally, 1 in 8 patients (12.6%) felt that the pandemic period had no impact on the treatment and diagnosis process.
Table 3 shows the associations between ITDP perceptions and selected individual characteristics of the respondents. Of the 8 individual factors analyzed, associations were statistically significant in 6 cases. The association was strongest with age, followed by gender and change in financial situation during the pandemic. Exclusively negative impacts were more often reported by men than women and by those aged 30–64 than the marginal age groups. The percentage of purely negative evaluations decreased as the family economic situation improved, as shown by the subjective evaluation index and changes during the pandemic (Table 3). The relationship between education level and employment was found to be weaker, but still statistically significant, to the disadvantage of better-educated and employed patients.
Table 4 presents the associations between ITDP perceptions and selected health indicators, also referring to medical services. Of the 7 individual factors analyzed, statistically significant results were obtained in 3 cases. The strongest associations were between the financing of private medical care (in favor of those paying with their own funds) and the treatment of the SARS-CoV-2 virus (to the disadvantage of those who were ill and self-treated). Partially positive opinions were more often expressed by those who had direct contact with healthcare professionals (ie, via inpatient visits, professional COVID-19 treatment).
Table 5 demonstrates the associations between ITDP perceptions and barriers to communication with HCWs that were related to COVID-19 pandemic restrictions, with statistically significant results observed in all 7 cases. The percentage of only negative ITDP evaluations ranged from 66.6% to 69.8%. Negative evaluations were also frequently reported in cases of no difficulties in communication caused by pandemic restrictions, but by a maximum of 51.6% of respondents. In contrast, the percentage of patients expressing mixed (or rarely, exclusively positive) opinions about the ITDP was always higher in the group that did not report difficulties compared to the group that reported them, reaching a maximum of 34.0%.
Table 6 shows the results of the multivariate binary logistic regression, which was estimated on the 1765 cases (94.5%) from the sample for which there were no missing data in the variables accepted for the final model. Of the 16 factors considered after the univariate analysis, half were proven to be independent predictors of exclusively negative ITDP perceptions. The factors are presented in the table in the order in which they were entered into the model. By far the strongest association was between ITDP perception and the greater focus on COVID-19 treatment than other health problems. Additionally, 3 of the 7 communication barriers that were previously shown to be significant in their association with ITDP perceptions qualified for the model, including remote contact (the second most important factor) and social distancing (the sixth factor). Among the demographic and social characteristics that were previously shown to be related to ITDP perceptions in the univariate analysis (Table 3), changes in family economic situation (the third most important factor), level of education (the fourth factor) and age (the eighth most important explanatory variable) qualified for the final model. This meant that 3 factors that were important in the univariate analysis did not enter the final model (ie, gender, occupation, and current family economic situation). Exclusively negative assessments of the ITDP were more likely among those whose family economic situation worsened during the COVID-19 pandemic, those with more than secondary education, and those of working age (with no clear differences between the 3 younger age groups). The highest odds ratio was reported for patients aged 18–29.
Among the factors related to health status and medical services provided during the pandemic, negative ITDP evaluations were most strongly influenced by self-funding private healthcare (ranked fifth) and remote consultations (ranked seventh). The risk of a negative ITDP assessment associated with the first of these factors was calculated by taking those who did not access private healthcare as the reference category as opposed to those who accessed private and public healthcare or co-funded private healthcare with self-funding (for example, as part of employee packages). However, in the estimated model, the quality of fit was quite low according to the Nagelkerke’s (pseudo) R-squared ratio of 0.139.
Discussion
LIMITATIONS AND STRENGTHS OF THIS STUDY:
The pandemic had diverse effects, negative impacts, and consequences from one country to another, so the results obtained in Poland should not be generalized to other populations. In addition, the data were from the last period of the pandemic and did not include longitudinal observations. Although we observed hypothetical cause-and-effect relationships, cross-sectional studies have limited power of inference. The nature of online surveys allows the results to be generalized to populations with higher digital competencies, although increases in these competencies and the development of e-health and m-health trends are considered to be positive effects of the pandemic. Additionally, the sampling method ensured a diversified cross-section of the population that was in line with the general structure, according to gender, age, education, and place of residence.
Satisfaction with the diagnosis and treatment process during the pandemic was assessed using a single questionnaire, which provided a picture of subjective evaluation. It would have been advisable to use more complex tools with verified validity and reliability values. The overall perception of the diagnosis and treatment process during the pandemic was assessed using a single item, which provided a picture of subjective evaluations. It was not possible to use an alternative composite tool with good relevance and reliability, which additionally takes into account the specific circumstances of our country. We realize that such an assessment does not reflect the changes in healthcare during the pandemic and the process of adapting to the constraints imposed by it. However, the advantage of using single-item measurements is that they are more time-efficient and enhance survey administration [59]. This was particularly important for our population-based survey, when we were eager to make sure that respondents would accept the length of the questionnaire. Using a short questionnaire may increase people’s willingness to complete and return the questionnaire [60] and enable more reliable results to be obtained. Simple measures of this type are acceptable when constructs are clearly defined and tightly scoped [61]. In our study, we assumed that both negative and positive impacts of the pandemic were possible. We therefore allowed for a divergence from highly polarized responses, giving those uncertain about the ITDP a chance to voice their opinions. It is also worth mentioning that we examined not only the distribution of ITDP in the population and its sociodemographic determinants, but also its relationship with perceptions of the restrictions introduced during the pandemic, the quality of communication with medical staff, and the association between ITDP and other factors related to health and medical services. Such analyses confirm the strong association of responses to a single question with independent evaluations of certain aspects of the treatment process during the pandemic.
Although a number of individual factors were considered, not all potential confounders were included. The association between ITDP perceptions and respondent health status was not confirmed, as the implementation of a population-based survey did not allow for an in-depth analysis of the health situation of the respondents. Generally, the reported opinions did not relate to a specific healthcare facility or a specific health problem, which provided an averaged view of patient experience across the 24 months of the pandemic.
However, we hope that the study’s strengths offset the above limitations. The study had the advantage of a large and geographically diverse sample. Additionally, we analyzed 22 factors that potentially affected patient assessments of the pandemic’s impact on the treatment and diagnosis process. The period of the study was also an advantage, as assessing the effects of the pandemic after months or years could be affected by recall bias. We hope that the conclusions of the above analyses inspire further studies or comparisons to other studies covering the post-pandemic period.
Conclusions
Patient evaluations of the ITDP are largely dynamic and multidimensional constructs, consisting of patient perceptions of their experience, as well as other factors. This study identified the key predictors of exclusively negative assessments of the ITDP, which included difficulties in communicating with medical professionals due to the focus on COVID-19 and deterioration in family economic situation during the pandemic. Patient satisfaction with received care is an important indicator that can help to develop measures to improve the quality of services provided, as well as promoting models of patient-centered care that implement humanizing medicine. It seems important to educate medical professionals regarding individual sociodemographic and cultural factors and the risks posed by crisis situations. Such issues should enter the framework of staff training due to their significant impacts on communication aspects and health education programs for different age groups and patients in order to improve health literacy.
Tables
Table 1. The characteristics of the patients (N=1860) treated during the COVID-19 pandemic in terms of health assessment and medical services received.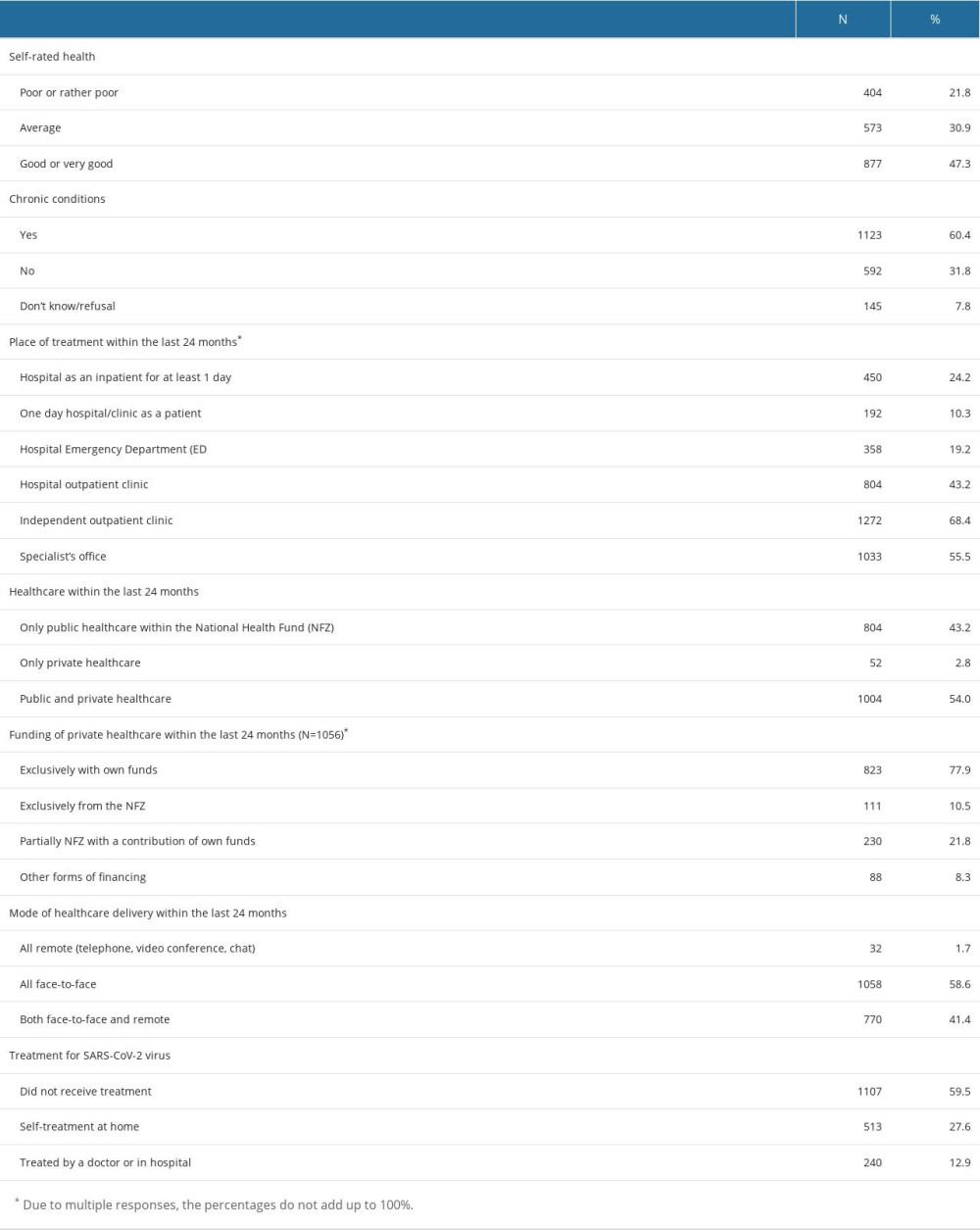 Table 2. The difficulties in communication with healthcare professionals and their causes from the perspective of patients (N=1860).
Table 2. The difficulties in communication with healthcare professionals and their causes from the perspective of patients (N=1860).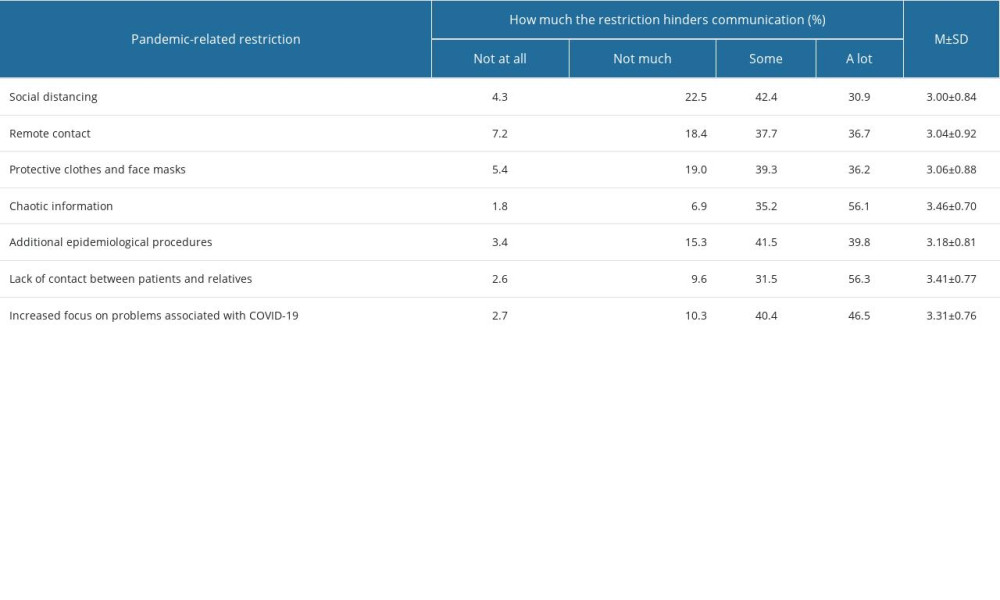 Table 3. ITDP perceptions according to selected demographic and social factors (N=1860).
Table 3. ITDP perceptions according to selected demographic and social factors (N=1860).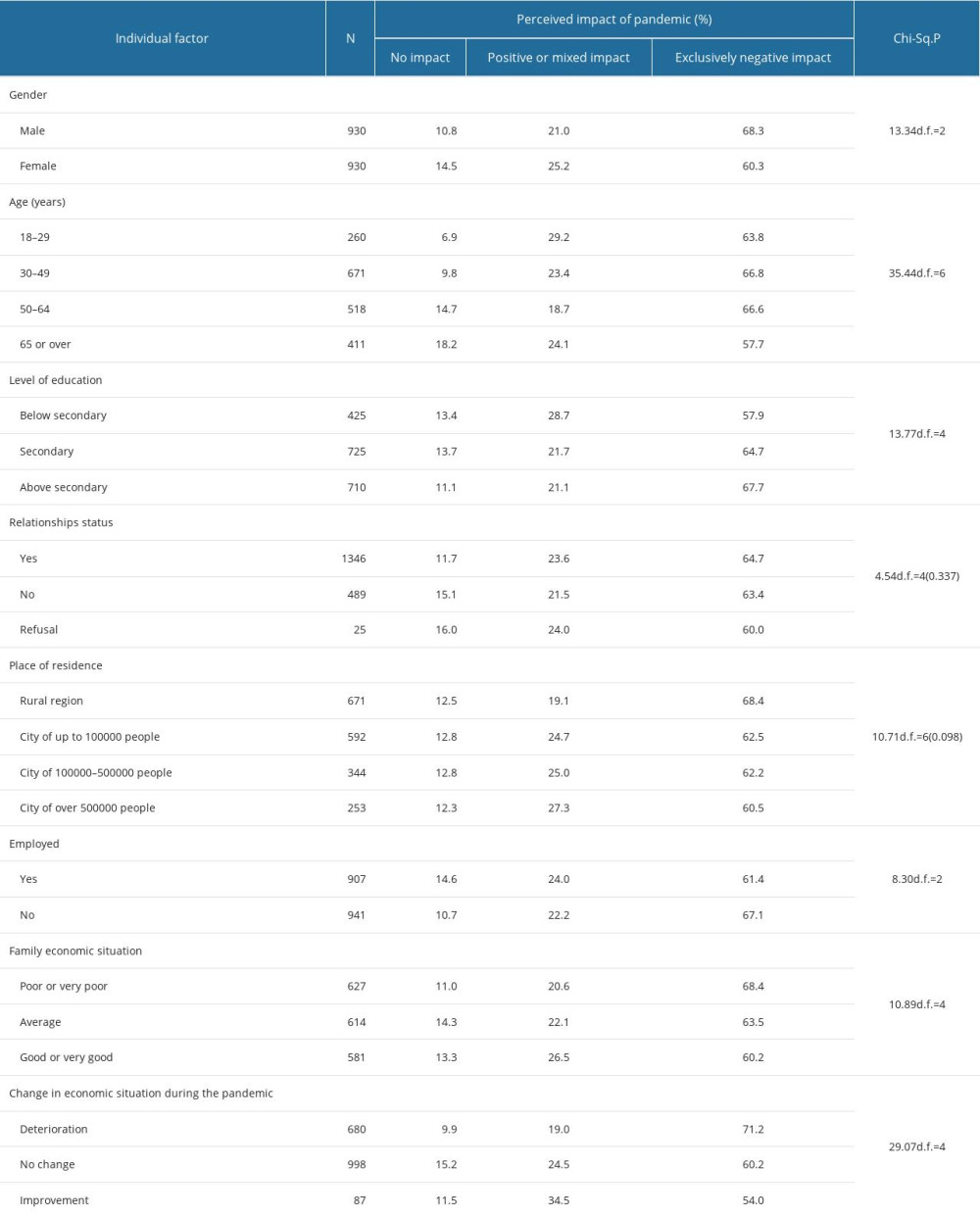 Table 4. ITDP perceptions according to selected health indicators (N=1860).
Table 4. ITDP perceptions according to selected health indicators (N=1860).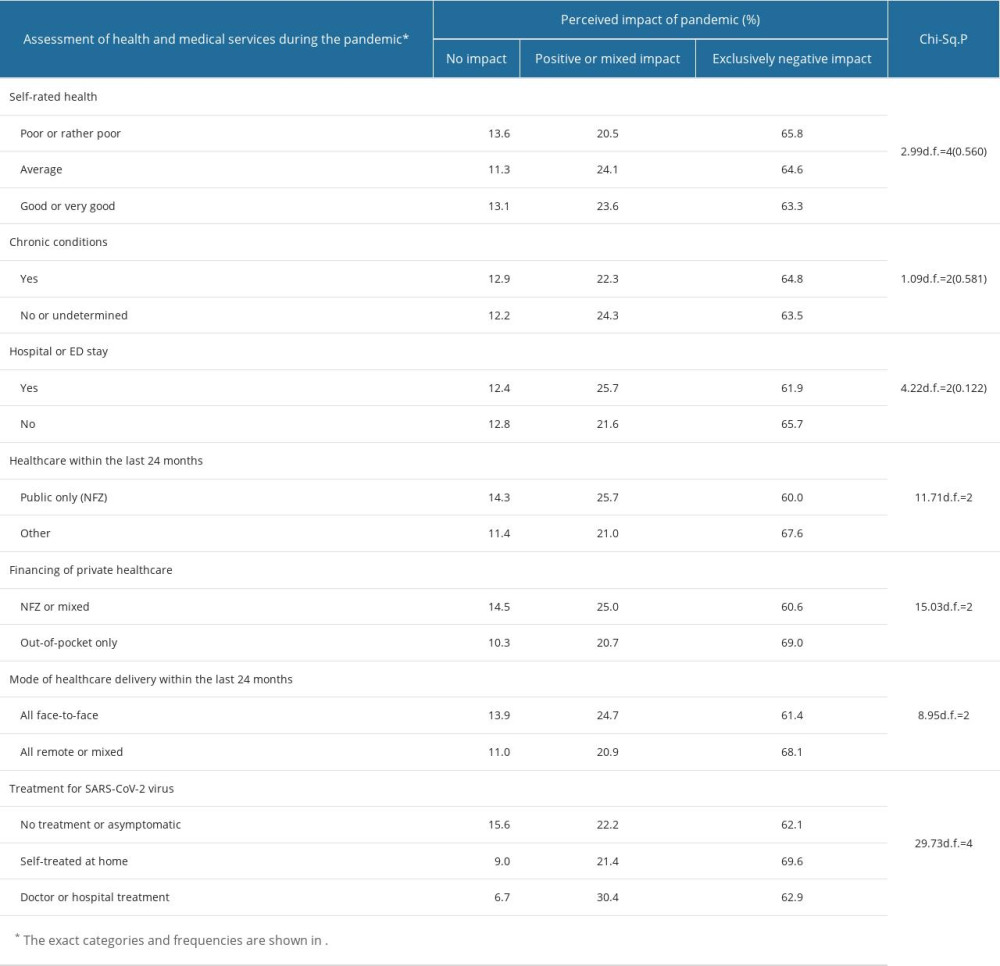 Table 5. ITDP perceptions according to pandemic-related difficulties in communication with HCWs.
Table 5. ITDP perceptions according to pandemic-related difficulties in communication with HCWs.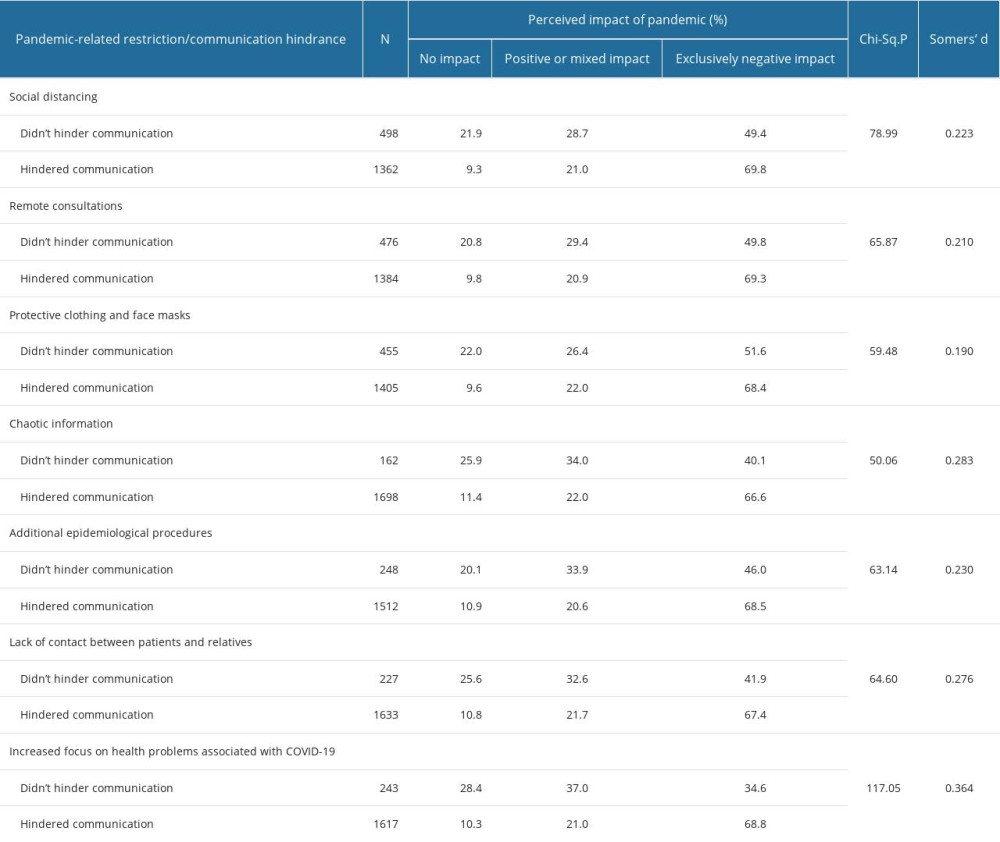 Table 6. The risk factors of exclusively negative ITDP perceptions, by order of importance when entered into the binary logistic regression model (N=1765).
Table 6. The risk factors of exclusively negative ITDP perceptions, by order of importance when entered into the binary logistic regression model (N=1765).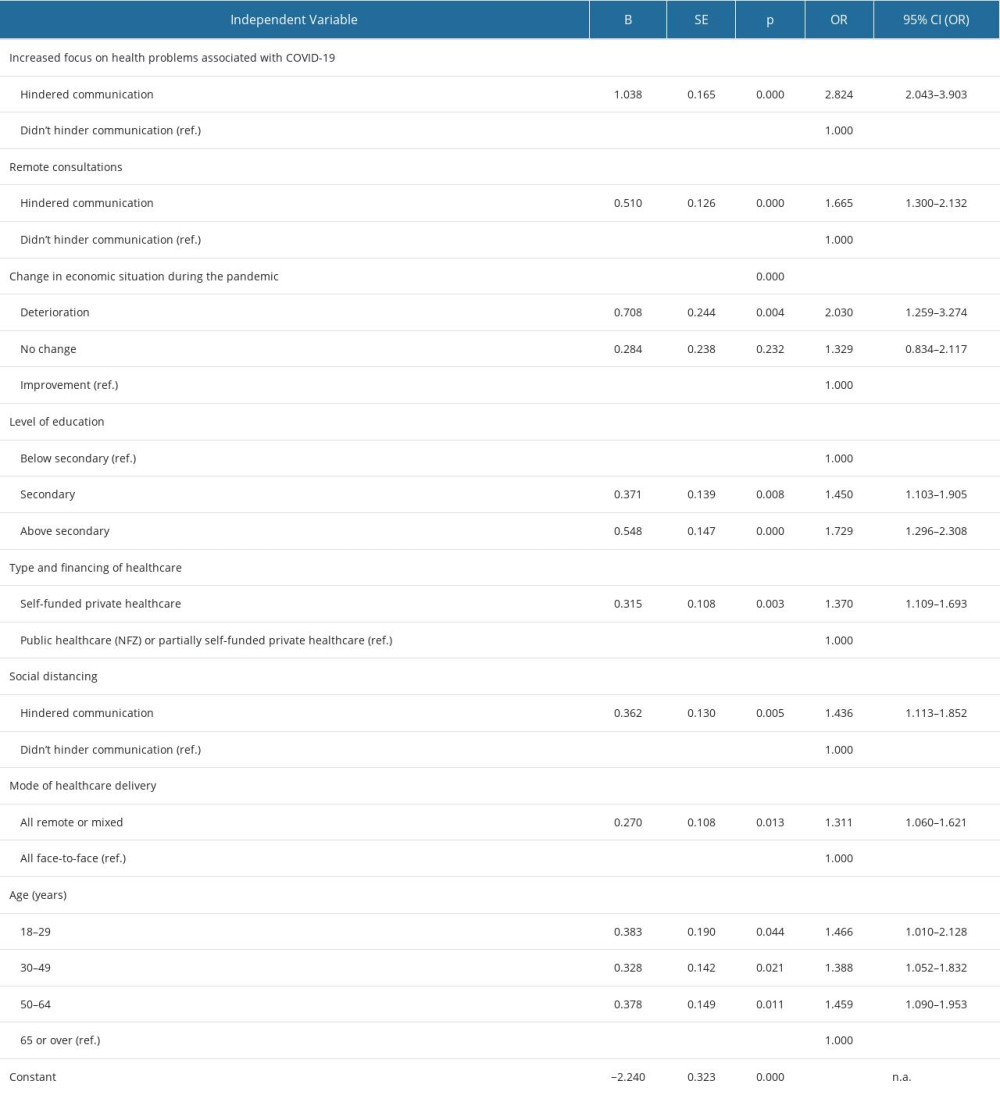
References
1. Caroppo E, Mazza M, Sannella A, Will nothing be the same again? Changes in lifestyle during COVID-19 pandemic and consequences on mental health: Int J Environ Res Public Health, 2021; 18(16); 8433
2. Szymborski J, Demographic implications of the COVID-19 pandemic: A public health perspective. Health and lifestyle: Economic, social and health implications of the pandemic, 2021, Wrocław, doi: 10.34616/142084 [in Polish]
3. Brooks E, Geyer R, The development of EU health policy and the COVID-19 pandemic: Trends and implications: J Eur Integr, 2020; 42(8); 1057-76
4. https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2
5. Murkowski R, Excess mortality in Poland during the COVID-19 pandemic in 2020: Polish Statistician, 2021; 66(7); 7-23 [in Polish]
6. https://www.nik.gov.pl/aktualnosci/bilans-po-pandemii-covid-19-debata-w-nik.html
7. Pillai S, Siddika N, Hoque Apu E, Kabir R, COVID-19: Situation of European countries so far: Arch Med Res, 2020; 51(7); 723-25
8. Robakowski P, Synoweć J, Poland’s health policy – what has changed in the era of COVID-19: Political Stud, 2020; 48(3); 85-106 [in Polish]
9. Healthy Future, 2021; 6, Warsaw, Ministry of Health https://www.gov.pl/attachment/4a9bd160-e052-4a52-8fd4-b7c546d556f8
10. OECD: European Observatory on Health Systems and Policies, 2022, Polska, Profil systemu ochrony zdrowia 2021, doi: 10.1787/b562ffe2-pl
11. Euro Health Consumer Index: Report, Health Consumer Powerhouse 2019, 2018 https://healthpowerhouse.com/media/EHCI-2018/EHCI-2018-report.pdf
12. Wojtyniak B, Goryński P: Health situation of the Polish population and its determinants 2022, 2022, Warsaw, National Institute of Public Health PZH – National Research Institute https://www.pzh.gov.pl/raport-sytuacja-zdrowotna-ludnosci-polski-i-jej-uwarunkowania/
13. : Decree of the council of ministers of March 30, 2021 on the National Health Program for 2021–2025; 2
14. Ruth L, Alongi J, Robitscher J: Confronting the health debt: The impact of COVID-19 on chronic disease prevention and management https://www.healthaffairs.org/do/10.1377/forefront.20210914.220940
15. Balasuriya L, Briss PA, Twentyman E, Impacts of the COVID-19 pandemic on nationwide chronic disease prevention and health promotion activities: Am J Prev Med, 2022; 64(3); 542-58
16. : Patients’ problems in the face of the COVID-19 epidemic – Report of the Patient Ombudsman, Warsaw, 2020 https://www.gov.pl/web/rpp/problemy-pacjentow-w-obliczu-epidemii-covid-19
17. Center for Public Opinion Research (CBOS): Use of health benefits and insurance, Warsaw, 2020; 9 http://www.cbos.pl/SPISKOM.POL/2020/K_098_20.PDF
18. Wyrzykowska M, Evaluation of nursing care according to patients: Pielęg Chir Angiol, 2007; 1; 3-10
19. Yeh J, Nagel EE, Patient satisfaction in obstetrics and gynecology: Individualized patient-centered communication: Clin Med Insights Women’s Health, 2010; 3; CMWH.S5870
20. Stewart M, Brown JB, Donner A, The impact of patient-centered care on outcomes: J Fam Pract, 2000; 49(9); 796-804
21. Ambigapathy S, Rajahram GS, Shamsudin UK, How should front-line general practitioners use personal protective equipment (PPE)?: Malays Fam Physician, 2020; 15(1); 2-5
22. Samarasekara K, ‘Masking’ emotions: Doctor–patient communication in the era of COVID-19: Postgrad Med J, 2021; 97(1148); 406
23. Benbenishty JS, Hannink JR, Non-verbal communication to restore patient–provider trust: Intensive Care Med, 2015; 41(7); 1359-60
24. Nwoga HO, Ajuba MO, Ezeoke UE, Effect of COVID-19 on doctor-patient relationship: Int J Community Med Public Health, 2020; 7(12); 4690
25. Kaul P, Choudhary D, Garg PK, Deciphering the optimum doctor–patient communication strategy during COVID-19 pandemic: Indian J Surg Oncol, 2021; 12(S2); 240-41
26. Gopichandran V, Sakthivel K, Doctor-patient communication and trust in doctors during COVID 19 times – a cross sectional study in Chennai, India: PLoS One, 2021; 16(6); e0253497
27. Izdebski Z, Mazur J, Furman-Kwiatkowska K: Humanizing the treatment process and clinical communication between patient and medical professionals before and during the COVID-19 pandemic, University of Warsaw Publishing House [in press]
28. Dubey S, Biswas P, Ghosh R, Psychosocial impact of COVID-19: Diabetes Metab Syndr, 2020; 14(5); 779-88
29. Duan L, Zhu G, Psychological interventions for people affected by the COVID-19 epidemic: Lancet Psychiat, 2020; 7(4); 300-2
30. Williams S, Tsiligianni I, COVID-19 poses novel challenges for global primary care: NPJ Prim Care Respir Med, 2020; 30(1); 30
31. Kouri A, Gupta S, Yadollahi A, Addressing reduced laboratory-based pulmonary function testing during a pandemic: Chest, 2020; 158(6); 2502-10
32. Farrell S, Schaeffer EK, Mulpuri K, Recommendations for the care of pediatric orthopaedic patients during the COVID-19 pandemic: J Am Acad Orthop Surg, 2020; 28(11); e477-e86
33. Usak M, Kubiatko M, Shabbir MS, Health care service delivery based on the Internet of things: A systematic and comprehensive study: Int J Commun Syst, 2020; 33(2); e4179
34. Fekadu G, Bekele F, Tolossa T, Impact of COVID-19 pandemic on chronic diseases care follow-up and current perspectives in low resource settings: A narrative review: Int J Physiol Pathophysiol Pharmacol, 2021; 13(3); 86-93
35. Birkmeyer JD, Barnato A, Birkmeyer N, The impact of the COVID-19 pandemic on hospital admissions in the United States: Study examines trends in US hospital admissions during the COVID-19 pandemic: Health Aff, 2020; 39(11); 2010-17
36. Whitwell K, Maynard R, Barry N, Strategic planning and response to COVID-19 in a London emergency department: Emerg Med J, 2020; 37(9); 567-70
37. Janke AT, Jain S, Hwang U, Emergency department visits for emergent conditions among older adults during the COVID-19 pandemic: J Am Geriatr Soc, 2021; 69(7); 1713-21
38. Monkman H, Kushniruk AW, Parush A, Lesselroth BJ, Information chaos: An adapted framework describing citizens’ experiences with information during COVID-19: Stud Health Technol Inform, 2021, IOS Press, doi: 10.3233/SHTI210630
39. Huth EJ, The information explosion: Bull N Y Acad Med, 1989; 65(6); 647-61 discussion 662–72
40. Klerings I, Weinhandl AS, Thaler KJ, Information overload in healthcare: Too much of a good thing?: Z Evid Fortbild Qual Gesundhwes, 2015; 109(4–5); 285-90
41. Rücker F, Hårdstedt M, Rücker SCM, From chaos to control – experiences of healthcare workers during the early phase of the COVID-19 pandemic: A focus group study: BMC Health Serv Res, 2021; 21(1); 1219
42. Lewnard JA, Lo NC, Scientific and ethical basis for social-distancing interventions against COVID-19: Lancet Infect Dis, 2020; 20(6); 631-33
43. Hart JL, Turnbull AE, Oppenheim IM, Courtright KR, Family-centered care during the COVID-19 era: J Pain Manag, 2020; 60(2); e93-e97
44. Davidson JE, Aslakson RA, Long AC, Guidelines for family-centered care in the neonatal, pediatric, and adult ICU: Crit Care Med, 2017; 45(1); 103-28
45. Maaskant JM, Jongerden IP, Bik J, Strict isolation requires a different approach to the family of hospitalised patients with COVID-19: A rapid qualitative study: Int J Nurs Stud, 2021; 117; 103858
46. Wu MS, Watson R, Hayat F, What do people hospitalised with COVID-19 think about their care? Results of a satisfaction survey during the first wave of COVID-19 in Liverpool: Future Healthc J, 2021; 8(1); e70-e75
47. Wunadavalli LT, Satpathy S, Satapathy S, Patient satisfaction scale for hospitalized COVID-19 patients: Development and psychometric properties: J Patient Exp, 2022; 9; 237437352210867
48. Mills EC, Savage E, Lieder J, Chiu ES, Telemedicine and the COVID-19 pandemic: Are we ready to go live?: Adv Skin Wound Care, 2020; 33(8); 410-17
49. Valentino LA, Skinner MW, Pipe SW, The role of telemedicine in the delivery of health care in the COVID-19 pandemic: Haemophilia, 2020; 26(5); e230-e31
50. Gogia SB, Maeder A, Mars M, Unintended consequences of tele health and their possible solutions. Contribution of the IMIA Working Group on Telehealth: Yearb Med Inform, 2016(1); 41-46
51. Kendzerska T, Zhu DT, Gershon AS, The effects of the health system response to the COVID-19 pandemic on chronic disease management: A narrative review: Risk Manag Healthc Policy, 2021; 14; 575-84
52. Alsabeeha NHM, Atieh MA, Balakrishnan MS, Older adults’ satisfaction with telemedicine during the COVID-19 pandemic: A systematic eeview: Telemed J E Health, 2023; 29(1); 38-49
53. Satpathy S, Wundaville LT, Satapathy S, A systematic review of patient satisfaction scales and their applicability to COVID-19 hospitalized patients: Gaps and emerging needs: J Patient Exp, 2022; 9; 237437352210791
54. Etter JF, Perneger TV, Validating a satisfaction questionnaire using multiple approaches: A case study: Soc Sci Med, 1997; 45(6); 879-85
55. Ryu S, Fan L, The relationship between financial worries and psychological distress among U.S. adults: J Fam Econ Issues, 2023; 44(1); 16-33
56. Sitzia J, Wood N, Patient satisfaction: A review of issues and concepts: Soc Sci Med, 1997; 45(12); 1829-43
57. Shinde M, Kapurkar K, Patient’s satisfaction with nursing care provided in selected areas of tertiary care hospital 1: International Journal of Science and Research (IJSR), 2014; 3(2); 150-61
58. Cerda AA, García LY, Factors explaining the fear of being infected with COVID-19: Health Expect, 2022; 25(2); 506-12
59. Allen MS, Iliescu D, Greiff S, Single item measures in psychological science: A call to action: Eur J Psychol Assess, 2022; 38(1); 1-5
60. Wanous JP, Reichers AE, Hudy MJ, Overall job satisfaction: How good are single-item measures?: J Appl Psychol, 1997; 82(2); 247-52
61. Fuchs C, Diamantopoulous A, Using single-item measures for construct measurement in management research: Conceptual issues and application guidelines: Die Betriebswirtschaft, 2009; 69(2); 195-210
Tables
Table 1. The characteristics of the patients (N=1860) treated during the COVID-19 pandemic in terms of health assessment and medical services received.Table 2. The difficulties in communication with healthcare professionals and their causes from the perspective of patients (N=1860).Table 3. ITDP perceptions according to selected demographic and social factors (N=1860).Table 4. ITDP perceptions according to selected health indicators (N=1860).Table 5. ITDP perceptions according to pandemic-related difficulties in communication with HCWs.Table 6. The risk factors of exclusively negative ITDP perceptions, by order of importance when entered into the binary logistic regression model (N=1765). In Press
06 Mar 2024 : Clinical Research
Prevalence and Variation of Medical Comorbidities in Oral Surgery Patients: A Retrospective Study at Jazan ...Med Sci Monit In Press; DOI: 10.12659/MSM.943884
08 Mar 2024 : Clinical Research
Evaluation of Foot Structure in Preschool Children Based on Body MassMed Sci Monit In Press; DOI: 10.12659/MSM.943765
15 Apr 2024 : Laboratory Research
The Role of Copper-Induced M2 Macrophage Polarization in Protecting Cartilage Matrix in OsteoarthritisMed Sci Monit In Press; DOI: 10.12659/MSM.943738
07 Mar 2024 : Clinical Research
Knowledge of and Attitudes Toward Clinical Trials: A Questionnaire-Based Study of 179 Male Third- and Fourt...Med Sci Monit In Press; DOI: 10.12659/MSM.943468
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952